-
Andrew Taylor Still founder of osteopathy
Osteopathy
The British Institute of Osteopathy was set up in 2002 and was built upon the great tradition of the osteopathic approach to therapeutics.
For any therapeutic to survive, it has to evolve to take account of the ever-changing clinical setting. This does not mean adopting the medical narrative and trying to make osteopathic technique fit – which I call ‘Osteolite’ – it means evolving the narrative to make it relevant in the modern clinical setting.
The current clinical setting is very different to the times of early osteopathy. Nowadays patients self-medicate, rarely now do patients understand the value of fever or rest and stress management. What we present here is a brief overview of where osteopathy has come from. This shows the roots of the pathway that has led directly to the new online course ‘Fast Track to Better Practice’ and a new evolutionary narrative – drawing on our roots, to make those brilliant simple early ideas time now relevant.
-
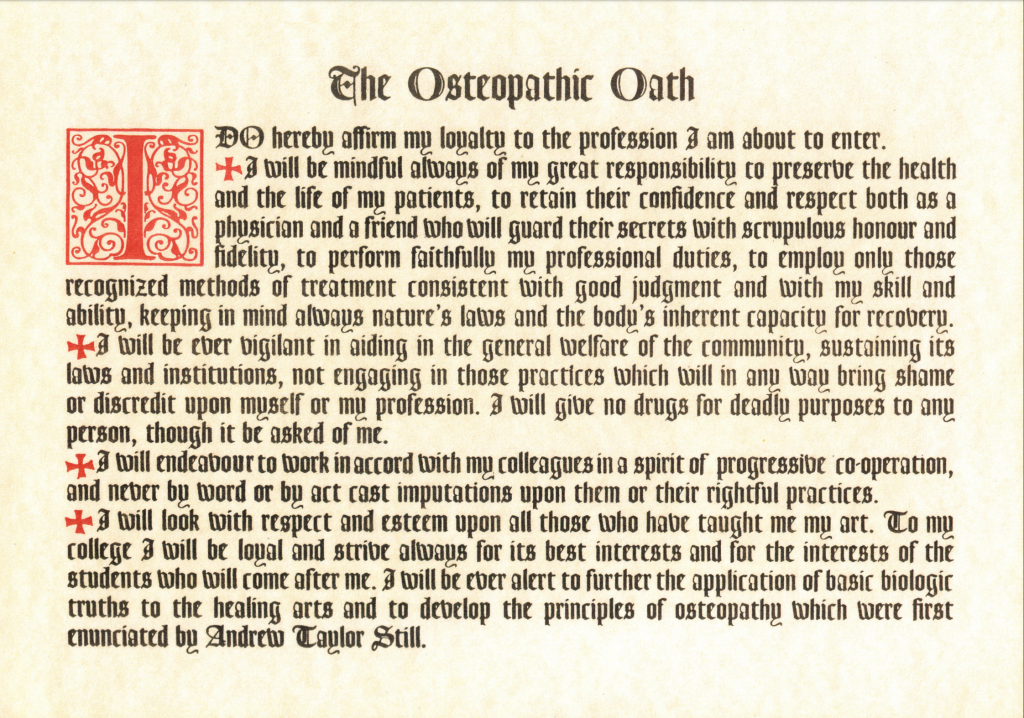
The osteopathic oath
The Osteopathic Oath, that was written by A T Still, is a derivative of the Hippocratic Oath. This used to be taken by all Osteopaths who received a diploma on graduating. Hippocrates was not the father of modern medicine; he was the father of Natural Hygiene. Within the Osteopathic Oath are a number of key principles that show direct links connecting osteopathy to the roots of Natural Hygiene.
This may be why the Hippocratic Oath is now optional for medical doctors, because none of these ideas have any connect to modern medicine. The following ideas underpin Osteopathy:
1. Keeping in mind nature’s laws and the body’s inherent capacity for recovery
2. I will give no drugs for deadly purposes
3. I will be ever alert to further the application of basic biologic truths to the healing arts and to develop the principles of osteopathy which were first enunciated by Andrew Taylor Still.
The British Institute of Osteopathy’s greatest developmental journey and message is to have reconnected with the narrative of Natural Hygiene – because without this narrative its technique has no value. Evolving the osteopathic approach to take account of the modern clinical setting has also been part of the journey. If we are to stay Osteopaths, in Still’s words ‘we must develop the principles of osteopathy’.
-
So what was early osteopathy?
‘The word, osteopathy, comes from two Greek words, osteon, bone, whose meaning is clear, and pathos, whose meaning is not always so clear, especially in this connection.
In Greek we find two words contrasted as are up and down, in and out; ethos, meaning an outgoing expression, and pathos, an incoming impression. The root meaning of pathos should therefore be taken as in the word sympathy “sensitive with” or telepathy “sensitive at a distance”, and not as in pathology which is a derived meaning in that which is almost a reversal of the original significance of the word.
Etymologically the name osteopathy is correct, meaning the influence of the bones in relation with disease, causation and cure, not bone disease or bone pain. Osteopathy then means osteo (bone), pathy (incoming effects from). The “incoming effects from bones” when disorder exists among them, was the first subject developed by Dr Andrew Taylor Still and his followers.
This study led directly to the second Osteopathic principle ‘natural immunity from disease stems from structural integrity’, two fundamental discoveries around which osteopathy is built.’
From The Theory of Osteopathy by Ernest E Tucker DO and Perrin T Wilson DO 1936
It’s interesting that the meaning of the word pathology has been changed in modern times to mean ‘the study of disease products’. There are many incidences where the re-branding of words has been used to hide the actual wisdom, insight and knowledge of the true roots of language.
-
The two first osteopathic principles were:
1. ’The rule of the artery is supreme and from its disturbance marks the second, minute and hour that disease starts.’ A T Still,
This led directly to:
2. Natural immunity to disease stems from structural integrity Quote from A T Still
Interesting to note that Still observed that the processes of disease involved disturbances in somatic factors, not distinctly external causes, and these revolutionary ideas lay at the heart of osteopathy’s founding principles.
Structural integrity also extends into the ability of the body to bring balance and homeostasis through all of its systems – like a Biome. This means that all structures are fit for function. In order to be able to adapt, the body has the capacity to adjust, within its best limits, to stay alive and vital. When we lose the ability to adapt and adjust – this is where osteopathy as a therapeutic can step in.
Osteopathic treatment is concerned with the process of restoring adjustment to the body by identifying and removing obstructions to health. (This does not mean the isolated cracking of joints, rubbing of isolated stiff bits or knots, which is Osteolite)Some modern terms for the word adjustment might be ‘restoring homeostasis’ or allowing balance back to the body. Health and un-health are both natural phenomena and the body does not go wrong, it does the best it can to ‘go right’.
-
What is osteopathy?
The osteopathic approach is a constitutional approach. The therapist approaches the problems it has to solve, by considering the body as a whole, not a set of unrelated parts.
Apart from acute combative trauma, many of the problems we are presented with are often degrees of compensation. A ‘twist here’ leading to ‘strain’ elsewhere, irritation in the viscera producing pain in the limbs. An Osteopath looks for the total context when solving problems which means we study ‘relationships’ not ‘differences.
Many patients are not well because of years of well meaning palliative treatments that have effectively obstructed the body from cleaning and real repair.
The problems are seen as obstructions to the health of the patient, rather than focusing on what may have gone wrong.
-
Not focusing on symptoms alone
Osteopathic treatment is about opening up the whole field of diagnosis and considers all the interactive relationships of the body. When we make a constitutional diagnosis, we look at the whole context of the presenting problem, instead of just focusing on the presenting symptoms.
For example, a patient with low back problems could have ‘viscero somatic referred symptoms’ which often occurs with constipation and menstrual disturbances. Attempting to treat the back pain alone with just painkillers denies the patient an opportunity to address the real causes. Any underlying issues thus not addressed, could develop into a chronic problem.
Just like in building work, a crack in a wall tells an Architect that the foundations may have slipped, putting a patch over the crack and doing nothing else is likely to make the crack spread. ’This is how the acute is turned into the chronic and ultimately the degenerative.
Howard Beardmore DO
-
The body is a vital organism – a biome
The body is able to assimilate nutrients and incorporate them into a living the body. This means that the body can vitalise matter and organise it into an intelligent living biome.
So, if we are to having any meaningful stability in our treatment method, directed at re-balancing disturbances in the patient, we have to engage in the totality of the problem, not just parts of it.
Constitutional Osteopaths approached solving clinical problems not as diseases in their own right, but as the natural consequences of obstructions to health. Of course in the acute combative trauma focusing on symptoms makes complete sense, Osteopaths recognise that. But most people are not acutely unwell, they are suffering from years of symptomatic suppression, which builds a huge load into the system. The constitutional approach has a lot to offer these patients because it looks for the cause, instead of loading yet more palliation into the system.
-
Disease or un-health, normal or abnormal?
So the idea that ‘diseases’ are isolated entities, or pathologies, in their own right, is not always true. Early Osteopaths like Ernst Tucker DO felt that we needed a new diagnostic. He would classify deviations from health in terms of the clinical adaptations in the physiology through the neuro-endocrine system; rather than use the vocabulary of orthodox medicine which had become distorted, eclectic and confusing.
If we are to approach therapeutics from a constitutional perspective, we need a narrative that reflects how we make a diagnosis and treat our patients and understand the functions of the body as a biome. for example: Constitutionally the immune system is a waste recognition and excretion system, if we obstruct its efforts to keep us ‘clean’ we start to produce symptoms.This is not pathology, it is normal immune system functioning like the oil warning lights coming on the dashboard, it is telling us to take action. We cannot just pull the light bulb out and expect a return to health!
Symptoms in the body can be explained as a physiological reaction to toxicity. This toxicity is effectively retention of our own waste products under the actions of chronic stress hormones, but can also be external poisonings from poor diet or toxic environment too.
In the new online course, a deeper discourse on the importance of the constitutional narratives on inflammation and immune function and health can be explored. Exploring the constitutional immune system -
Some early writers thoughts on the constitutional nature of therapeutics
Each one of these writers has observed some key concepts regarding natural therapeutics. Here is a basic summary of ideas and contributions that have influenced the evolution of osteopathy from earlier times.
Hippocrates, was the first person to note that the spine was important in therapeutics, so it is not a new idea.
‘It is necessary to know the nature of the spine, what it’s natural purposes are, for such a knowledge will be required for many diseases’ Hippocrates 400BC
“It is far more important to know what person the disease has, than what disease the person has.” ― Hippocrates 460BC
‘There are no diseases – only obstructions to health’ Hippocrates 460BC
‘There are no diseases, only obstructions to cleaning and healing’ Howard Beardmore DO 1996
-
Tucker Wilson DO The Theory of Osteopathy 1936
‘There are two organized agencies for combating disease or for conducting the defense of the body against unfavourable influences – the nervous and endocrine systems’
Tucker DO, wrote a book called the ‘Endocrine Brain’ which attempted to reclassify diagnosis and describe conditions as neuro endocrine disturbances – rather than distinct and separate medical pathologies.
Although this was a step away from the restrictions of using medical language it still kept us tied to the idea that we needed to label presenting conditions as distinct and different. A true constitutional approach recognises that when the body is well adjusted it is well. When it is not well adjusted it is unwell. Naming the consequence/pathology is academically interesting but does nothing to help the patient in the final analysis.
-
Louisa Burns
At the A T Still Research Institute, Sunny Slope Laboratories USA, there were many attempts to do research on the nature of the osteopathic spinal lesion. Burns tended to focus on very specific vivisection experiments and establish a relationship between spinal lesioning and specific disease prodromes. Burns was convinced that using what amounted to medical RCT studies on animals would be the only way to convince orthodox medical researchers that osteopathy had value.
Although Burns was able to demonstrate repeatable methods and results that seemed to prove her point, the medical establishment largely dismissed her work which spanned over many decades. Her seminal work was a book that detailed and catalogued decades of her work:
‘Pathogenesis of visceral diseases following vertebral lesions’ Burns 1948
In the opening chapters to the book Burns says ‘We have discovered the missing link between physiology and pathology’
Although Burns proved her point scientifically, she did not include the constitutional context in her testing model. Her spinal lesioning was artificially induced, not the consequences of normal living and as such what she tested was ‘lesion here, get an effect there’. For research to have practical value in the real world of patients we have to test our ideas and theories with real patients and every patient is different – effectively a control of one.
If we are to truly test somatic factors, in poor health considerations; we cannot leave out all the other constitutional factors that give context to the presenting problems. We have to test all somatic influencers, simultaneously, or we are not testing Osteopathy.
Just taking spinal lesioning alone – dehydration, lack of rest, nutrition, lifestyle, and many more constitutional factors can all affect the effects and potency of the outcome. We cannot reduce testing of osteopathy to an intervention of ‘one’.
Burns demonstrated that vivisection cannot ever be used as a research base for the constitutional approach because it is testing something else. Burns and others, tried to demonstrate that there was a ‘neurological basis’ for the osteopathic lesion but what they showed was only a connection between spinal injury and visceral consequences. Because they used a medical reductionist rational in an attempt to ‘test’ and ‘research’ Osteopathy by default they didn’t test Osteopathy!
So this is not a dismissal of the work of Burn’s in anyway at all, it is a constructive critique acknowledging the role of spinal lesioning as one factor in poor health, but not the totality.

-

Irvin Kim Korr
Korr was very aware of Burns but Korr did his experiments upon human patients! Not vivisection, but using a method that tested the electrical skin resistance patterns on patients who had many varied visceral conditions. He demonstrated using dermatomal mapping how various visceral conditions could be recorded electrically and results could be repeated.
He made two really profound statements from his years of great work that certainly helped focus the attention on constitutional approaches to therapeutics rather than segmental observations.
Sustained sympatheticonia as a factor in disease – was a ground breaking theory, linking the various states of disease and lesioning as degrees of ‘sympathetic phenomena’.
2. Korr observed that although adjusting spinal lesioning had a profound effect on quite remarkable pathology, it was difficult to stabilise the adjustments. They would not ‘hold’.
Korr transformed our understanding of lesioning and it’s effects on the constitution but realised you had to do more than attempt to ‘correct’ lesions in isolation – osteolite!
Korr did focused on segmental lesioning, but made honest statements about the limitations of not approaching research from a constitutional perspective. This is may be why using a general treatment bodywork routine has a more stabilising/holding effect on lesioning because it adjusts arch relationships rather than segments. Diagnosing a segmental block and hitting it makes no sense for the patient.
-
Edward Long Fox
Fox wrote one of the first books that linked all disease processes having a connection to disturbances in the sympathetic system i.e. adrenal dominance. In the opening paragraphs of his book written in 1885 he states:
The three most important points that the consideration of the sympathetic seems to be to illustrate, are 1. The marvellous effect of reflex action in health and disease in connection with this system. 2. The exquisite mutual dependence of the various portions of the nervous system – cerebral, spinal, and sympathetic – on each other. 3. The fact that, in spite of this mutual dependence, the sympathetic, under the conditions of lesion of brain or spinal cord, is enabled within certain limits to act independently.’ Consulting physician to the Bristol Royal infirmary ‘The influence of the sympathetic in disease 1885
-
Dare to be different, so many would rather be orthodox than right’
– Henry Fryette
Henry Fryette
‘Dare to be different, so many would rather be orthodox than right’
Fryette, another American Osteopath, gave us a context to understand how the spine moves as a whole, rather than segmentally. His work was extensive, self-reflective and honest. He knew spinal segments moved in groups, depending on the starting posture and devised classifications to describe how the spine lesioned into various compensatory patterns.
When Fryette did early experiments on cadavers observing spinal lesioning, he soon realised that there was no vertical loading and this perverted the results. It was only when he observed contextual movement in real subjects and then tested spinal movement; that he was able to correctly report how the spine moves when lesioned.
He saw spinal lesions as compensations, rather than just problems that needed solving. Fryette gave us:
1. Segmental lesioning is necessary to allow movement in the rest of the spine.
2. Segments do not lesion in isolation. it is the pre-existing nature of the spinal arch relationships that determines how the spine moves in side-bending and flexion and extension
3. A contextual way to understand spinal lesioning
Again, whilst Fryettes work was ground breaking it was his final conclusions that were the most useful. It is a mistake to think we can treat spinal lesioning by identifying facet blocks and cracking them – without considering anything else. Fryette made some very useful observations about contextual movement but did not give us a rational for treatment.
Film 3 in the online course explores constitutional biomechanics and represents 23 years of thought process behind making stable adjustments. Making Biometric adjustments constitutionally
-
Early Osteopaths did not study disease
Studying or adopting the orthodox classification of the separateness of disease, borrows terminology from a different discipline to the constitutional approach and often leads to confusion.
If the original observations of A T Still of ‘natural immunity’ and ‘structural integrity’ were to mean anything, then physiology – or how the body works – had to be taught from a perspective that looked at the relationships, rather than the differences in the way the body worked. Physiology is a reflexive phenomenon not a set of isolated specialisms. It is capable of sharing stresses and strains to limit damage when we are under pressure.
Often in patients with chronic constipation we find a chronic cough, or poor skin conditions as the body tries to develop compensatory ways to eliminate waste. Do we stop the cough, put cream on the skin or deal with the underlying cause?
It is the narrative that you use that gives potency to the approach, not the technique’ and nowhere is this more important than in therapeutics.
Many excellent books were written by the A.T Still institute explaining the osteopathic philosophy on physiology, some of which still exist. There are no books on the philosophy of orthodox medicine, only books on protocols, ethics and legality.
-
They studied health
Studying health instead of disease made sense. If you logged all the physiological similarities in patients with gastrointestinal ulcers for example and those without the similarities in diet, posture, spinal lesions, habits, lifestyle etc would make it pretty obvious what the maintaining factors could be and even the cause.
This may look obvious and begs the question, why doesn’t orthodox medicine acknowledge or recognise this as a logical approach. If you look at orthodox medical training you will see that its tendency towards specialism, reductionism and symptomatic suppression is the problem. Most medical student’s introduction to training involves spending the first year dissecting a dead body to find out how it works! Considering we are working in the field of the living, why not start by studying life?
In the current Covid phenomena, no one seems to be studying people who ‘have it’ and then recover with no sequale? Where is the science in that? No one is studying people living with people who do not ‘catch it’, why not? Is it really that hard to convince medical science to study people who are well and vital?
A gastrointestinal specialist is only able to describe ‘perversions’ that are local and distinct to the gastrointestinal tract (GIT). This is fine if there is an obstruction or an acute trauma injury; the advances in trauma surgery have saved many lives.
-
Local or reflex?
If however, the cause is not local but reflex, then this approach fails. Symptomatic relief or palliation is the consequence, an attempt to moderate the tissues causing the symptoms is tried, and the local diagnosis leads to local treatment. Many chronic ailments are classified as ‘auto immune’ i.e. the body is attacking itself and the only treatment is to turn off the immune system. What about the idea that the body may in fact being trying to repair a problem but is not being supported to do so?
What if the immune system was doing it’s job of dealing with diseased tissue by trying to clean and repair it?
The consequence from the ‘continual palliation of symptoms’ as a therapeutic – is to pave the way to chronic and degenerative diseases, because constitutionally we are suspending the maintenance contract. Too often these ‘symptoms’ are either the body’s attempts to raise alarm or actual cleaning/repair events. The sequalae of degeneration, from long term suppressive approaches, as in the ‘atopic’ pathway; is now well known.
Howard Beardmore DO
What is an osteopathic lesion?
The osteopathic lesion is not ‘a bone out of place’ but any obstructions to physiological processes. This may include – irritation, inhibition, deficiency or excess that may, if left unaddressed, lead to a state of unhealth. This can include diet, lifestyle, posture, mental and physical trauma, poisoning. Any method that is directed only at managing the symptomatic picture, by palliating symptoms and suppressing natures attempt to clean will only open the pathway to chronic and degenerating lesioning.
A key feature of lesioning is the degree to which the sympathetic adaptive state is left ‘in charge’. The main thrust of treatment is to relieve the body of this sympathetic overdrive so that health can return to easy normal.
Howard Beardmore DO

-
The osteopathic Lesion
The description is deliberately trans-dimensional and not definitive, because the constitutional osteopathic approach acknowledges all of the interdependent and symbiotic correlations that are continually part of the homeostasis or balance of health.
This is ostensibly about supporting the immune system’s function to negate the effects of toxaemia by re-establishing elimination, upbuilding, cleaning and repair.
This is infinitely variable, so it is impossible to be prescriptive about treatment. Every patient is a control of 1 and it is their obstructions and enervation’s that are the true field of therapeutic diagnosis, specific to them. Lesioning is as specific to them as the treatment required to restore them to health.
There can be no prescriptive treatment protocols for specific conditions – that is the biggest fallacy medicine throws at the patient. If you chase pathology you are chasing death. Seek what keeps us alive not what stops us dying! Howard Beardmore DO
-
Diseases or obstructions to cleaning?
There are no ‘diseases’ or ‘cures’ only obstructions to immune system processes. Osteopaths understood from a clinical, physiological and philosophical perspective that the only true ‘disease’ is toxaemia or the retention of waste. These wastes maybe from external or internal origins.
The focus of toxaemia peculiarises symptoms and then names an illness by the symptoms peculiar to the toxic focus – and the symptoms are often the attempts at ‘cleaning/repair’ expressed via various actions of the immune system. Howard Beardmore DO
Examples might be suspended secretions in the gall bladder can lead to gall stones, in the kidney it is kidney stones, in the salivary glands it is salivary duct stones.
From this you could extrapolate that there are at least three states of toxaemia, acute chronic and degenerative. Being able to place the patient correctly in terms of the toxic state is the key to making a constitutional osteopathic diagnosis.
The ‘cohorts of patients’ additional learning resource along with the ‘fields of diagnosis’ and the ‘constitutional immune system’ are a great way to visualize where your patient is on the road to recovery Place your patient on the road to recovery

-
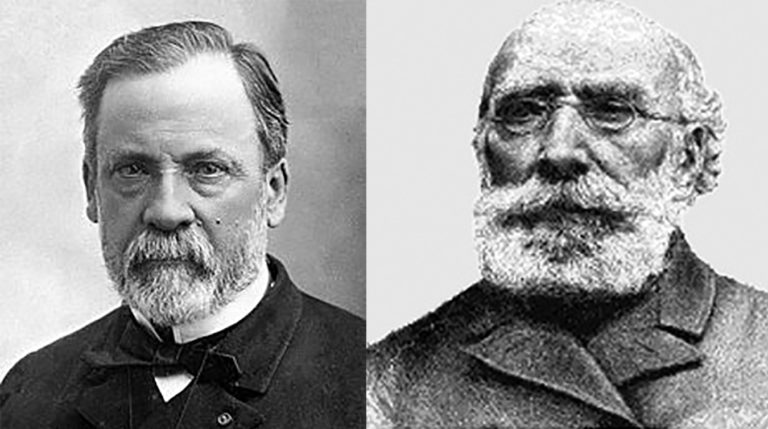
Louis Pasteur or Antoine Bechamp?
It is an orthodox ‘notion’ that diseases are ’caused’ by germs and viruses based on the work of the 19th Century Frenchman Pasteur. Interestingly on his deathbed he is quoted as his last words to have said:
‘Bernard the germ is nothing the soil is everything’. Louis Pasteur – sourced from Bechamp or Pasteur E Douglas Hume 1923
However, another microbiologist called Antoine Bechamp at the time said:
‘If man goes down the therapeutic route of killing the germ it does not bode well for mankind for diseases are born of us and within us’ Antoine Bechamp. It is interesting to note that in John Lewis’s autobiography of A T Still he noted that Still had read the works of Bechamp and one wonders if, like Henry Lindlahr – Still recognised how close Bechamp was to the osteopathic understanding of health and Natural Hygiene?
Film 1 explores the background to the constitutional Osteopathic approach and how it has been evolved to make sense in a modern clinical setting. It traces our work back to Hippocrates, through A T Still to the current day. To know your roots is to know your work
-
The unhealth state is not abnormal
Susceptibility to the unhealthy state, is a natural consequence of a disturbed immune system and its cleaning functions. This usually leads to toxaemia, or the retention of waste.
The retention of waste in any tissue is naturally irritative and the consequent inflammation is a normal event. this is the stimulus that starts the cleaning process. This is followed by elimination, restoration and repair. When there is a focus of toxaemia, the whole body may get involved by way of a systemic fever and the process can be quite vitriolic.
Instead of classifying diseases as distinct and different, which other therapies do, early Osteopaths studied the similarities between the degrees of compensations that occur, as a reaction to toxemia. This compensatory process is a normal function of our immune system when health drifts towards the unhealthy state.
For example, when the kidneys get into trouble, the skin will start to excrete, to support – and the patient will smell of urine. If the liver starts to struggle, we see yellowing of the skin, this is not disease as such, it is supportive compensation; a normal immune system adaptation to keep us alive. It is not ‘deficiency in deodorant’
What a constitutional Osteopathic approach can therefore offer, is an alternative diagnostic narrative to the differential reductionist approach. What the Constitutional Osteopathic approach does not do is borrow a medical diagnosis and attempt to suppress the symptoms using different techniques.
For example, bronchitis is not ‘irritation of the bronchioles’ but is in fact cleaning of the lung!
-
Attempting to treat constitutional conditions locally leads to more problems
For patients who are treated locally by ‘modifying tissues’ to just ‘kill the germs’ the immune system ‘cleaning’ will keep on returning until either the patient expires, or the cleaning stimulus of toxemia is gone.
Every time we just ‘kill germs’, but doing nothing about why they are there, the germs will adapt to cope with the new more toxic environment.
Sometimes the body will move the waste to another organ, usually deeper. This may explain the ‘atopic pathway’ that moves eczema from the skin to the lung in asthma and to the bowel in anaphylactic bowel conditions as each ‘disease’ is symptomatically relieved by stronger and stronger methods of palliation, and pushed further into the constitution.
A clinical effect of steroids is to produce a reverse transport of waste metabolites from the blood back into the tissues; this is how they moderate the symptoms of a ‘cleaning’ event so successfully. But you cannot keep putting off the cleaning audit, long term steroid use leads eventually to tissue degeneration.
-
But if we allow the constitution to do it’s work
The patient who is assisted to finish the cleaning with good therapeutic support, however, does not get a repeat performance. Unless, of course, the lung requires a new phase of cleaning or the patient lapses back into enervating habits.
Recovery from years of palliation takes time, effort and skilled mentoring and the practitioners who are still able to do this are becoming scarce. You cannot learn this kind of work on a modular course alone, with no mentored practice. At some point the osteopath in training, will experience managing a patient with a healing crisis and you will need a good narrative to be able to support the patient and understand what is happening.
Being a patient yourself is the best learning curve because it makes the learning real. If the patient is ever to believe they are in good hands the practitioner cannot have academic experience alone.
-
Learning from clinical evidence
Patients who were ill were studied in terms of their constitutional adaptations rather than just describing the presenting symptoms. The approach was to ‘get behind the symptomatology’ rather than study ‘disease’ in isolation. Many old osteopathic books would list lesion patterns present in illnesses, highlighting some of the adaptations in physiology, which sought to dispel much of the mystery of disease pointing to a new way to treat the sufferer.
In a sense, discovering somatic lesioning and attempting to correct it opened up a whole new therapeutic field that had never been considered before.
What was missing from the purely Osteopathic narrative however, was the constitutional rational for understanding how the immune system produced many symptoms, as a normal part of it’s function to keep us clean and repair us.
From the texts of Natural Hygiene writers the overproduction of mucus from any part of the body was understood as nature’s attempt at ‘local tissue washing’ when ‘general washing’ has failed.
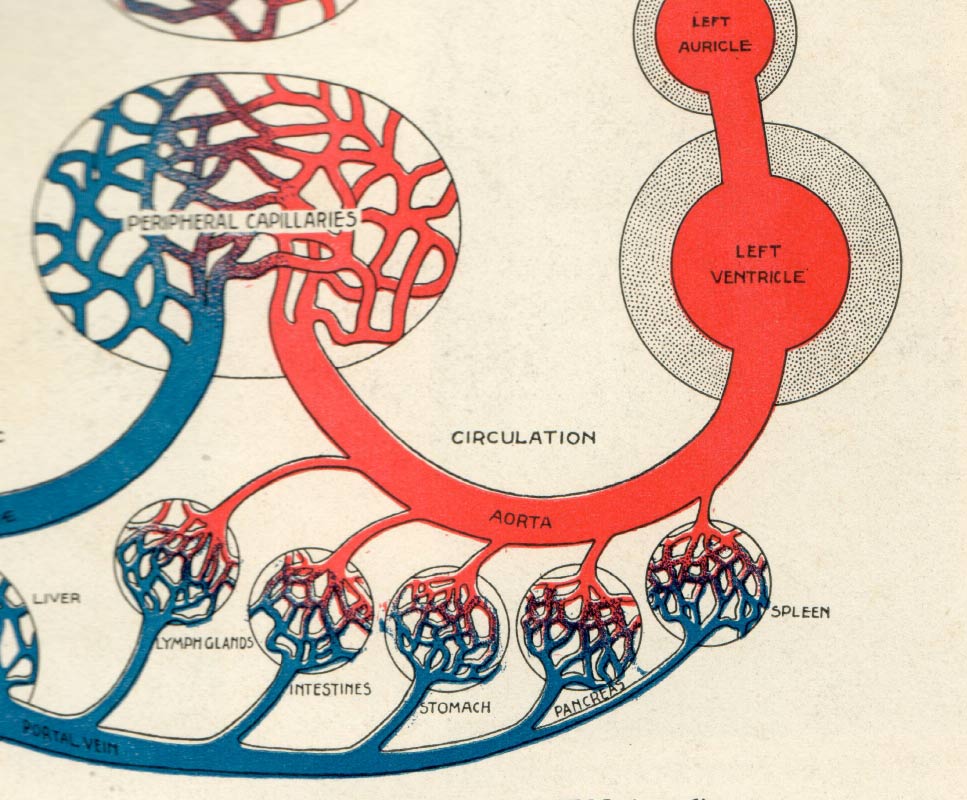
Arterial blood brings nutrition to the tissues the venous lymphatic, mucous and digestive systems remove waste thus preventing toxemia, the build-up of waste. Any deficiency of action in any one or more of these areas can lead to supportive excesses in the remaining areas. Seeing these relationships, rather than differences is a core part of a constitutional approach in the modern clinical setting.
-
Health is the ability to adapt both in good times and bad
If the lymphatic and venous systems or the cleaning organs can’t cope then the nearest mucous membrane to the focus will go into overdrive. This is known as hyper-physiology. The constitutional Osteopath looks elsewhere for the failing, recognises the adaptation, removing obstructions to the flow of circulation and thus renders the compensating hyper-physiology unnecessary.
Context is everything!
These normal immune system compensations are what an orthodox approach calls ‘disease’ and it’s symptoms require suppressing. Effectively the suppression of cleaning is what turns an acute toxemia to a chronic one and finally a degenerative one. This is because the restorative part of the immune system is unable to complete repair.
Many so called ‘disease prodromes’ were thought to be the direct result of years of suppressive palliative treatments by early writers and you can see their point.
-
Disease is not a mystery science
Orthodox approaches often imply that the causes of virtually all ‘diseases’ are unknown. This has led some to ‘blame’ poor design of the body as the culprit. Modern orthodox approaches often conclude that study of the genome will unlock the mystery of illness and lead mankind to some kind of nirvana of endless health. When we are able to ‘redesign’ the bits that have failed us and implant new bits no one will need to be ill. However well marketed, the hydroponic tomato does not taste, look or smell like an outdoor variety.
Also the 20 year Genome study that looked at twins with genetic markers considered to be associated with various pathology traits failed to prove this to be true.
The discovery of antibiotics has not relieved man of infection, quite the opposite. The World Health Organization lists antibiotic resistance as the number 1 threat to global human survival. Recently the Nobel peace prize was won by a man who discovered how to inhibit the action of RNA, that is turn on and off the action of cells. The idea is that you will be able to manipulate cellular activity and therefore turn off disease.
Personally I think this will bring us closer to ‘degeneration’ without any recourse to recovery because it is the accumulation of suppressed colds, influenza and immune system cleaning events that keeps us well; not disinfectant. The prevalence of chronic disease modern man is currently experiencing must be due in part to the unprecedented access to over the counter palliation. Without any ‘pathway’-cleaning/ healing events for the life of the patient – the body will just go straight to terminal illness. In the words of Antoine Bechamp on germ killing as a therapeutic approach:
“If man goes down the therapeutic route of killing the germ, it does not bode well for mankind’
Sourced The Eye of Bechamp by Hector Grasset 1913 translated by Jocelyn C Proby DO MRO.
-
Osteopathic research
There is a large amount of research to support the constitutional Osteopathic approach, but some of it is conveniently dismissed by ‘modern’ researchers as ‘out of date’. Currently you cannot use any work that is over ten years old in a literature review – an important part of any research.
This needs challenging because it means that progress cannot take into account old ideas, clinical evidence and any approach that challenges the status quo. Modern science cannot claim to be whole if it limits the field of exploration to only the present. Most brilliant discovery happens in practice not in planned research models.
Currently there is a tendency to only invest in research that has a projected marketable product at the end. This means that the Constitutional Osteopathic approach is not popular to shareholder led research; it would however be an inspirational basis for reforming the NHS because it is low tech, patient-centered and much cheaper than exponential, maintenance medication regimes.
The loss of independence in the NHS and further privatisation can only lead to more corporate planning and thus a narrowing field of therapeutic availability for the public.
This is why the British Institute of Osteopathy has among its aims the establishment of a free research laboratory whose only interest is the re-validation of the basic biological truths that underpin both the art, science and practice of constitutional therapeutics. It will not use vivisection or genetic manipulation because we need to study health in the human not disease in animals.
Why randomised controlled trials (RCTs) don’t work
Orthodox medicine demands that any therapeutic has to satisfy the ‘gold standard’ of randomised controlled trials. There have been many failed attempts to do this with osteopathic treatments, an understanding of why these attempts will always fail needs to be discussed, because a lot of time is being wasted, with good intent; that could be put to better use.
One reason why randomised controlled trials or RCTs so often fail to produce any evidence to support alternative approaches to maintaining health is because RCTs were designed to test pharmaceutical interventions, only allowing one variable at a time. They were also about treating pathology, which Osteopaths don’t do. As was explained earlier, there is no disease as such, only obstructions to healing and repair.
How do you find a cohort of test subjects with exactly the same constitution, life story, diet, partner, job……… and then introduce a variable and test it? This alone is a total fallacy.
Because RCTs can only deal with one variable and the constitutional osteopathic approach is multifaceted, the osteopathic practitioner is forced to reduce his treatment to only one intervention – to fit the trial model. This is an immediate fail, what is the point of claiming to do ‘osteopathic research’ if you are not including all the variables as part of the study? Including all the variables is a core part of the true Osteopathic approach.
This effectively means that almost all the modern attempts at research on Osteopathy are not actually testing osteopathy, but they are proving the ineffectiveness of RCTs on testing the validity of symbiotic, multifaceted, constitutional approaches.
-
Appeals to false authority
The danger here is that fake osteopathic RCT’s then produce a database of flawed research that is used incorrectly to undermine the true clinical value of the constitutional Osteopathic approach. For example, the medical practitioner thinks that what we do is ‘crack joints’ in isolation to relieve symptoms.
Trials have been set up to test the effectiveness of this idea, calling it ‘manipulative medicine’ on ‘non-specific back pain’. ‘Non-specific’ back pain for a start is a ridiculous concept, how can any pain be ‘non-specific?’ The nature of the cause of pain is a core requirement of an Osteopathic diagnosis and absence of this knowledge before treatment is tantamount to malpractice.
Test operators are then asked to ‘crack’ a particular joint against someone who does ‘sham joint cracking’, whatever that is? The trial results are announced and usually the outcome is that ‘sham cracking’ is no different to ‘isolated cracking’. They are right, they have proved that osteolite treatment is comparable to sham treatment.
No context means no treatment!
This is a bit like someone deciding that ‘surgery is cutting holes in people’ and with no guiding principles I make ‘non-specific’ holes in people and compare the outcome with random stabbing and declare that there is no difference.
It is also nigh on impossible to find hundreds of patients for a trial, all with the same condition – and more importantly the same history of health and the same constitution. If the trials focused on the diagnostic approach that constitutional Osteopaths used and measured the outcomes, the true potency of this approach would be obvious.
There is nothing more patient centered than a constitutional diagnosis.
What is a constitutional Osteopathic diagnosis based upon?
In the fields of osteopathic diagnosis, an osteopath considers factors that have led to the failure to adapt rather than stimulating or forcing the body to accept the state of unhealthy by suppressing symptoms.
This will involve doing an audit of many fields, including lifestyle, diet, posture, occupation, hobbies, sport, activity, rest cycles…………. In a sense unless we ‘diagnose’ from the total context of the patient, we are not making a constitutional diagnosis.
A patient, who has a slight twist in the pelvis, may produce symptoms of pain and swelling in the knee, as a referred strain. They may have a twist in the pelvis as a viscero somatic reflex reaction from their chronic constipation or uterine problems.
A reductionist approach would entail the patient visiting someone different for the knee, bowel/uterus, pelvic strain which might mean three or four different treatments.
Just treating the pain in the knee as an illness ignores the intelligence of the body’s feedback, saying ‘don’t use it’ and then may lead to ‘wearing’ of the knee structure. Rather like if the tracking is ‘out’ on your car the tyres will wear on the inside and just replacing the tyres will result in the strain being moved elsewhere.
The twist in the pelvis may be due to impaction in the bowel from a poor diet, which would move the centre of gravity producing a counter strain on the posture. There could be a myriad of reasons why the problem has presented symptoms in the knee and the key to a successful result depends on being deductive with reasoning rather than differential.
Constitutional resolution of this kind of case means no problems in all of those fields and would encompass one integrative constitutional diagnosis.
If you want to learn more about how to use Osteopathic principles in a modern clinical setting, why not go to film 2 Using Osteopathic Principles in a modern clinical setting -
Classifications of unhealth
Adaptations from health can be classified into four main groupings:
- Acute. Natures attempts at cleaning and may include fever, sweating, boils and skin eruptions, diarrhoea, vomiting, overrun of mucus, inflammation, organ discharges and bleeding to name a few. Used to be referred to as ‘vicarious’ elimination.
- Sub-acute. Just below the level of symptoms
- Chronic. Nature’s failed attempts at acute brought about by either not enough vitality to produce an acute or the result of continued suppression of the acute process.
- Degenerative. Final stage of chronic. The body is unable to muster an acute event. The continual saturation with waste metabolites eventually leads to the break down of tissue.
So when making a diagnosis from a constitutional Osteopathic perspective the main focus is to assess the toxic state and ascertain whether the patient is acute, chronic or degenerative. The ‘reserve’ of the patient also needs consideration.
The reserve is the capacity of the patient to manifest the various cleaning crisis necessary for a return to full health, often leading to ‘preparatory advice’ to maximise the beneficial outcome of treatment.
Physiologically the ‘reserve’ could be measured by the degree of alkali buffering in the blood because this is directly called upon in the cleaning crisis to neutralise the acids of waste, into salts, thereby rendering the acids harmless and ready for excretion.
Howard Beardmore DO
-
The positive way forward
It could be so much cheaper and easier if we had a health service, rather than a disease management service and everybody was taught how to maintain their health. Rather like – we are all expected to be responsible for our financial affairs. Then we would only need an acute A and E for accident care, obstructive childbirth and injuries sustained in warfare.
Schools would teach children how to stay well and the chronic health care budget would evaporate.
-
‘The best solution to disease is health’
The greatest advances in public health have not been through drugs and vaccines, but through clean water, clean air, sanitation, transport for fresh food, and dealing with urban overcrowding.
In both prevention and treatment of disease, it is all too easy to overlook the basic things the body needs in order to be healthy. Yet these things should be central to the task. Hence most Osteopaths prefer a drug-free approach; instead placing the emphasis onto the body’s in-built healing mechanisms, and the basic necessities of life.
If you like the idea of working in a constitutional way, why not check out our online course
-
Events
Biometherapy & The British Institute of Osteopathy regularly hold events for both members and non-members. For further details on future events, click on the link below
Soon we will be announcing the beginnings of the Practical Days that compliment the online ‘Fast Track to Better Practice’ pathway.

Why train with the British Institute of Osteopathy?
Being a delegate of our Practical Courses at the British Institute of Osteopathy brings many benefits
- Part of a growing community of great Osteopathic practitioners you can refer others to
- A place to build your CPD based on Practically applied Osteopathic work
- ‘Learning with others’ BIO Delegate only webinars
- Practical training courses based on the evolved General Treatment approach
- BIO members mentorship scheme for clinical help with cases where you can contact members for help with cases, CPD and learning with others
Contact Us
- 13 New Road Reading Berkshire RG1 5JD
- howard@biometherapy.co.uk